

Introduction:
With the emergence of the Coronavirus Disease 2019 (COVID-19) as a global pandemic came the concern that it would adversely affect individuals with comorbid conditions. In sickle cell disease (SCD), the apprehension was largely driven by concerns that the disease causes chronic inflammation, organ dysfunction and a prothrombotic state, especially during a vaso-occlusive crisis. Our assumption and hypothesis was that SCD pathology would be exacerbated by SARS CoV-2 infection leading to higher rates of acute chest syndrome (ACS), venous thromboembolism (VTE), more robust inflammatory responses requiring ICU care and increased death rates.
Sickle cell trait (SCT) is frequently perceived as a benign condition; however, mounting evidence has shown that severe hypoxia (such as that seen in COVID-19 infection) can trigger sickle-related complication such as VTE, papillary necrosis and splenic infarcts and, in rare cases, ACS. In this retrospective analysis, we aimed to determine if sickle cell disorders (SCD & SCT) would confer poorer outcomes and/or increased mortality due to COVID-19 infection.
Methods:
Within the MedStar health care system there are 7,551 adult patients with a diagnosis of sickle cell disorder. We performed a retrospective chart review of all patients in the MedStar system with hemoglobinopathy and a lab-verified diagnosis of COVID-19 infection between March 1, 2020 and June 30, 2020. Sixty-one patients met our search criteria with 21 patients admitted to the hospital and 40 patients managed in the outpatient setting. Of the 21 patients admitted: 9 patients had sickle cell disease (Hb SS, Hb SC, Hb SB thalassemia) and 11 patients had sickle cell trait. One patient had HbC disease.
Results:
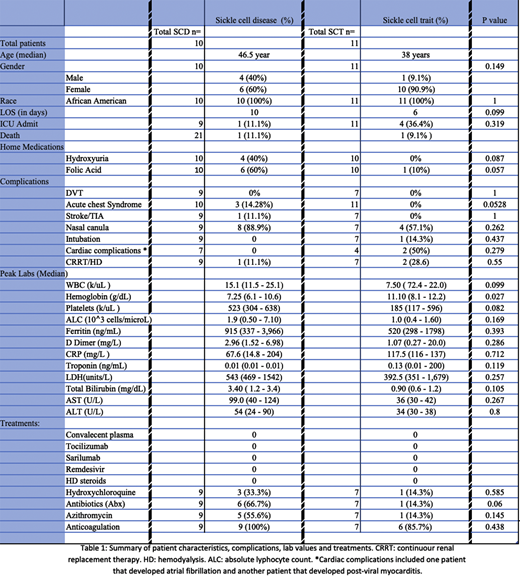
Results were analyzed by SCD genotype (Hb SS, Hb SC, Hb SB Thalassemia) versus the presence of a SCT. Due to the small sample size, statistical significance was not met in the variables. In the 21-patient cohort: 76.2% were female (60% of SCD and 90.9% of SCT) and 100% were African American. Median age was 46.5 years in the SCD group and 38 years in the SCT group. Length of stay was 10 days in the SCD group and 6 days in the SCT group. Mean peak white blood cell count and platelet count were significantly higher in SCD group (WBC: 15.1 k/uL vs 7.5 k/uL; p value 0.099. Platelets: 523 k/uL vs 185 k/uL; p value 0.082). Inflammatory markers were more elevated in the SCD cohort: mean Ferritin (915 ng/mL vs 520 ng/mL), mean D Dimer (2.96 mg/L vs 1.07 mg/L) and mean LDH (543 units/L vs 392 units/L). However, mean peak C-reactive protein (CRP) was higher in the SCT group (117.5 mg/L vs 67.7 mg/L). Admission to the intensive care unit (ICU) occurred in 11.1% with SCD & 36.4% with SCT and renal replacement therapy was required in 11.1% with SCD & 28.6% with SCT. Nasal cannula was required in 75% of patients (88.9% of SCD & 57.1% of SCT; p value 0.262) with only one SCT patient requiring intubation and mechanical ventilation whom later died. Two patients with Hb SS developed ACS, one of whom died. One patient with HbSC disease developed ACS and an acute cerebrovascular accident. No VTE or pulmonary embolisms were documented in this cohort.
Therapeutic drugs used in the cohort varied, with 43.8% receiving antibiotics (other than Azithromycin), 37.5% receiving Azithromycin and 25% receiving Hydroxychloroquine. None of the patients received convalescent plasma, steroids, tociluzumab, sarilumab or remdesivir. Anticoagulation was used in 93.8% of the patients (13.3% of which were in therapeutic doses).
Conclusions:
Sickle cell disease diagnosis did not seem to influence response to COVID19 illness when compared to age-matched individuals with SCT. The number of patients with sickle cell disease admitted to the hospital after contracting SAR CoV2 infection was also remarkably low. These findings were, in general, unexpected. Although the inflammatory biomarkers were generally higher in the patients with SCD, more patients with SCT were admitted to the ICU and required renal replacement therapy. The major drawbacks of the study are the small sample size and missing data points (lack of labs, lack of documentation, transfer to another facility) that did not allow us to draw statistical conclusions about the differences in the patients with SCD versus SCT. We were also unable to determine the influence of SCD severity and pre-existing organ complications on outcomes in COVID 19 disease. Additional studies with larger cohorts is warranted.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal